Introduction: The Invisible Bridge
Mechanical ventilation (MV) is frequently misunderstood by the public as a cure. In reality, it is a vital organ support and a bridge to recovery—a temporary replacement for the respiratory system that buys the body the most precious commodity in critical care: time. Understanding the history and education for a nurse anesthetist reveals a study in radical transformation.
The journey from the 19th-century ancestors of the ventilator to the microprocessor-controlled units of today is a study in radical transformation. We have moved from “large and cumbersome” airtight boxes that manually manipulated the atmosphere around a patient to intelligent, portable systems that utilize artificial intelligence to protect delicate lung tissue. For Certified Registered Nurse Anesthetist (CRNA), this evolution represents a shift from simply forcing air into a patient to a high-precision discipline of personalized medicine.
The “Tank Shock” Era: When Breathing Was Negative
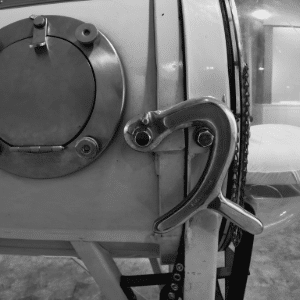
Before the era of modern intensive care, engineers and physicians relied on negative pressure to assist failing lungs. The concept gained traction in 1838 when John Dalziel designed the first “tank ventilator.” In this early iteration, the patient actually sat inside an airtight box—a position the sickest individuals often described as the most comfortable for breathing.
By creating a vacuum inside the tank, the machine lowered the ambient pressure around the thorax, creating a pressure differential that drew air into the lungs. This reached its cultural zenith with the “iron lung” developed by Drinker and Shaw in 1928. However, these machines introduced a lethal complication known as “tank shock.” The negative pressure caused blood to pool in the abdomen and legs, reducing venous return and frequently leading to fatal cardiac arrest. Because these machines required significant expertise to operate, the early foundations of Certified Registered Nurse Anesthetist (CRNA) education began to emphasize the dangers of mechanical interference with human physiology.
“These machines required significant expertise to operate and were dangerous for patients.”
1952: The Year the World Learned to Breathe Under Pressure
The global approach to ventilation underwent a seismic shift during the 1952 poliomyelitis epidemic in Copenhagen. Confronted with a staggering 87% mortality rate among paralyzed patients, Professor Bjorn Ibsen proposed a revolutionary alternative: abandoning negative pressure tanks for manual positive pressure ventilation delivered via tracheostomy.
The impact was immediate. By manually “bagging” air into the lungs, medical teams saw mortality rates drop from 87% to 40% instantly, eventually reaching 23% by the end of the epidemic. This transition was the catalyst for modern ICUs and the rigorous CRNA education requirements we see today. Ibsen recognized that the breakthrough wasn’t just the machine, but the accumulation of high-needs patients into a singular, dedicated area where experts could manage complex physiology in a concentrated environment.
Protect the Tissue: The Modern “Lung-Protective” Revolution
In contemporary medicine, the priority has shifted from simple gas exchange to the prevention of Ventilator-Induced Lung Injury (VILI). We now recognize that a “one-size-fits-all” approach can cause biotrauma by overstretching the “baby lung”—the small portion of aerated tissue remaining in a diseased or ARDS-afflicted lung.
Personalizing the Breath Modern clinicians focus on “personalized” settings, primarily through the monitoring of Driving Pressure (DP). Calculated using the formula DP = Pplat – PEEP, this metric provides a far more accurate indicator of volumetric lung strain than simple tidal volume.
Precision in this area is vital, and staying current via CRNA continuing education is essential for bedside safety. We also calculate Mechanical Power (MP), which represents the total energy transferred from the ventilator to the lung tissue. Precision in this area is vital:
- Experimental Threshold: In piglet models, an MP higher than 12 Joules/minute was found to lead to VILI.
- Clinical Threshold: In human clinical observations (recorded after ICU admission), an MP greater than 17 Joules/minute is independently associated with increased mortality.
Beyond the Lungs: Guarding the Heart and Diaphragm
Ventilation is a whole-body balancing act where the lungs, heart, and diaphragm must be managed as a single system. Because the ventilator increases intrathoracic pressure, that pressure is transmitted to the heart and great vessels, creating complex “heart-lung interactions.” Specifically, this can increase Right Ventricle (RV) afterload while reducing RV preload, potentially compromising the patient’s entire cardiac output.
Equally critical is the prevention of “myotrauma”—the injury or atrophy of the diaphragm. To preserve this primary muscle of breathing, we must avoid three specific failure states:
- Over-assistance: When the ventilator does too much work, the diaphragm weakens and undergoes myofibrillar atrophy.
- Under-assistance: Insufficient support forces the patient to exert excessive effort, causing muscle inflammation and proteolysis.
- Dyssynchrony: A mismatch between the patient and machine can cause “eccentric contraction,” where the muscle is forced to lengthen while attempting to contract, leading to significant damage.
To stay updated on these complex interactions and manage CRNA continuing competence, many professionals utilize their CRNA login to access the latest peer-reviewed articles and MAC Ed resources.
The Futurist’s Vision: AI and the “Wayfinding” Ventilator
By 2050, the role of the machine will shift from a passive tool to an active “wayfinding” partner. In this context, “wayfinding” represents a transition from simply predicting diagnostic labels to guiding the clinician through the entire clinical course in real-time. As technology advances, CRNA CEU requirements will likely evolve to include digital literacy and AI-augmented monitoring.
Future systems will feature “agnostic connectivity,” allowing ventilators, monitors, and infusion pumps to share data across interoperable platforms. AI will analyze entire datasets of airflow and airway pressure to predict respiratory distress before it occurs. We also anticipate innovative materials for non-invasive ventilation (NIV) interfaces and advancements in High-Flow Nasal Cannula (HFNO) technology to provide more comfortable, effective support.
“From now on, synergy of human knowledge and wisdom (human neurons), and AI (artificial neural networks) to achieve diagnostic excellence must coexist.”
Conclusion: The Ethical Horizon
Mechanical ventilation has moved from a desperate last resort to a sophisticated instrument of precision medicine. We have evolved from crude manual bellows to AI systems capable of monitoring microscopic energy transfers within human tissue.
As machines become capable of managing themselves, the role of the human clinician will evolve toward higher-level ethical and clinical oversight. The future of the ICU will depend on the wisdom of multidisciplinary ethical teams who must decide not just if a machine can support a life, but how that support serves the patient’s ultimate quality of existence. In an era of automated breathing, human wisdom remains the most vital sign of all.
Log in to CRNAeducation.com today to access articles hand-selected by CRNAs, for CRNAs.
Email: support@crnaeducation.com